I've been a bit tardy in blogging due to work commitments, but The Paper Mask has made it into Grand Rounds again!
This week's Grand Rounds is hosted by Prudence MD.
Make sure you check it out!
Thursday, November 29, 2007
Friday, November 23, 2007
PagingDr is Back
PagingDr is back up and running, less a few hundred posts.
There is a great deal of talk about what happened. I am not passing judgement on anyone involved.
I have received this email and I post it verbatim, with permission from the author.
(Click to Expand)
Edit 24/11/07: The relevant thread has since been deleted from PagingDr.
There is a great deal of talk about what happened. I am not passing judgement on anyone involved.
I have received this email and I post it verbatim, with permission from the author.
(Click to Expand)
Edit 24/11/07: The relevant thread has since been deleted from PagingDr.
Wednesday, November 21, 2007
PagingDr is down
Unfortunately something has gone wrong with the PagingDr forums. I don't know what, but my eyelid is starting to twitch from withdrawal symptoms.
This is from Bel at Audaci.net
Hopefully it will be up and running soon.
This is from Bel at Audaci.net
Breaking my silence to let you all know that the Paging Dr forum has been put into maintenance mode temporarily to protect the posts. A user deleted 400 posts in the space of nine minutes, and not just their own, which says to me they either don't know how to run a script properly or they're just malicious. Either way we don't care, we just don't want anymore deletions. The forum will come back up once we've spoken to Proboards and figured out how to protect its integrity. Would the other forum users with blogs also post this up so other forum users will know what's happened? We're not prepared to send a mass email just yet for other reasons.
Hopefully it will be up and running soon.
Monday, November 19, 2007
10 Years in Limbo
As a follow-on to a recent discussion thread over at PagingDr, I had cause to review the effect of the 10 Year Moratorium on Medicare Provider Benefits.
This has been a big deal because it effectively limits non-Australian Citizens or Permanent Residents from gaining access to Medicare Provider Benefits.
You may recall from the first instalment of my Mind the Gap Series that outside of the public hospital system the Federal Government funds medical services via the Medicare system (including the PBS and the Commonwealth Medical Benefits Schedule [CMBS]).
This renders the Federal Government extreme power and influence over who delivers medical care to the community via the allocation and restriction of Provider Numbers, and also how that care is delivered via limitations, restriction and conditions placed upon services before they are eligible for reimbursement via Medicare.
Note that this is a relatively roundabout method of control over medical practitioners. The Federal Government does not tell doctors what to do. They merely tell doctors that unless they do things in a specific way, satisfying Medicare guidelines and Ministerial Determinations, that their patients will not be able to have their medical costs reimbursed.
Therefore in theory it is not the doctor who is being punished, but the patient. Unfortunately, the doctor is the one that the patient sees face to face. The bills and invoices carry the doctors name. If the patient can't get money back from Medicare or their insurance company, it is the doctor they complain to, not the 17 year old counter chick at the Medicare office, or the faceless call-centre operator on the end of the phone line.
And if you are unfortunate enough to be one of the 90% of doctors that do not get payment upfront then you end up unpaid because the patient can't get their Medicare reimbursement.
What does this have to do with the 10 Year Moratorium?
Well, the 10 Year Moratorium is one of the limitations (along with Bonded Medical School Places) that the Federal Government applies to restrict access to Medicare benefits. It's purpose is to encourage doctors to enter and remain in the public hospital system, or to work in "areas of need" as defined by Medicare, brought in as part of John Howard's 1996 Provider Number reforms (More Info).
It applies to Overseas-Trained Doctors who migrate to Australia as well as non-citizens and non-permanent residents who commence studying medicine in Australia.
Basically if you fall into the target population, patients who see you in private (in your clinic or rooms) or on whom you operate in a private hospital will not have their medical costs reimbursed or subsidised by the Federal Government. In a system where patients are accustomed to paying little or nothing out-of-pocket this is tantamount to shutting these doctors out of the market, unless you do what the Government tells you to, and work where they tell you to work.
Fine, it's primary purpose is to encourage doctors into "areas of need". But what about non-resident doctors who gain their medical qualifications in Australia? These include full-fee paying students from overseas, as well as New Zealanders (who are on Special Category Visas) who study medicine in Australia. These students take up valuable medical school positions, but are discouraged from working in Australia for 10 years after their graduation, when they have careers they can easily go to in New Zealand and elsewhere.
Furthermore, they aren't banned from working in Australia - only from working outside the public hospital system. That means that they are free to pursue their specialist qualifications and postgraduate degrees (but GP trainees have to enter the Rural Training Program). After this, however, they have to go overseas or off to the bush (which increasingly means outer metropolitan urban fringes) to bide their time.
It seems a colossal waste of university and hospital resources to train people who can easily avoid the rest of their Provider Number limbo by heading overseas (and most likely never returning).
But then again, maybe the Department of Health knows what it's doing...
Exemption guidelines for doctors need fixing: report - The Australian
(Click to Expand)
GP shortage in outer suburbs: report - The Australian
(Click to Expand)

This has been a big deal because it effectively limits non-Australian Citizens or Permanent Residents from gaining access to Medicare Provider Benefits.
You may recall from the first instalment of my Mind the Gap Series that outside of the public hospital system the Federal Government funds medical services via the Medicare system (including the PBS and the Commonwealth Medical Benefits Schedule [CMBS]).
This renders the Federal Government extreme power and influence over who delivers medical care to the community via the allocation and restriction of Provider Numbers, and also how that care is delivered via limitations, restriction and conditions placed upon services before they are eligible for reimbursement via Medicare.
Note that this is a relatively roundabout method of control over medical practitioners. The Federal Government does not tell doctors what to do. They merely tell doctors that unless they do things in a specific way, satisfying Medicare guidelines and Ministerial Determinations, that their patients will not be able to have their medical costs reimbursed.
Therefore in theory it is not the doctor who is being punished, but the patient. Unfortunately, the doctor is the one that the patient sees face to face. The bills and invoices carry the doctors name. If the patient can't get money back from Medicare or their insurance company, it is the doctor they complain to, not the 17 year old counter chick at the Medicare office, or the faceless call-centre operator on the end of the phone line.
And if you are unfortunate enough to be one of the 90% of doctors that do not get payment upfront then you end up unpaid because the patient can't get their Medicare reimbursement.
What does this have to do with the 10 Year Moratorium?
Well, the 10 Year Moratorium is one of the limitations (along with Bonded Medical School Places) that the Federal Government applies to restrict access to Medicare benefits. It's purpose is to encourage doctors to enter and remain in the public hospital system, or to work in "areas of need" as defined by Medicare, brought in as part of John Howard's 1996 Provider Number reforms (More Info).
It applies to Overseas-Trained Doctors who migrate to Australia as well as non-citizens and non-permanent residents who commence studying medicine in Australia.
Basically if you fall into the target population, patients who see you in private (in your clinic or rooms) or on whom you operate in a private hospital will not have their medical costs reimbursed or subsidised by the Federal Government. In a system where patients are accustomed to paying little or nothing out-of-pocket this is tantamount to shutting these doctors out of the market, unless you do what the Government tells you to, and work where they tell you to work.
Fine, it's primary purpose is to encourage doctors into "areas of need". But what about non-resident doctors who gain their medical qualifications in Australia? These include full-fee paying students from overseas, as well as New Zealanders (who are on Special Category Visas) who study medicine in Australia. These students take up valuable medical school positions, but are discouraged from working in Australia for 10 years after their graduation, when they have careers they can easily go to in New Zealand and elsewhere.
Furthermore, they aren't banned from working in Australia - only from working outside the public hospital system. That means that they are free to pursue their specialist qualifications and postgraduate degrees (but GP trainees have to enter the Rural Training Program). After this, however, they have to go overseas or off to the bush (which increasingly means outer metropolitan urban fringes) to bide their time.
It seems a colossal waste of university and hospital resources to train people who can easily avoid the rest of their Provider Number limbo by heading overseas (and most likely never returning).
But then again, maybe the Department of Health knows what it's doing...
Exemption guidelines for doctors need fixing: report - The Australian
(Click to Expand)
GP shortage in outer suburbs: report - The Australian
(Click to Expand)
- Doctor Connect on Provider Number Restrictions for OTDs
- Health Insurance Act 1973 Section 19AB
- Student Doctor Forums (US) Discussion Thread
- Dept of Health & Ageing - Medicare provider number eligibility (section 19AA) - Temporary residents
- Dept of Health & Ageing - Medicare provider number eligibility (section 19AB) - OTDs
- GP Registrars Australia Website on the 10 Year Moratorium
- Tropical Medicine Training Website (source of image below)
Sunday, November 18, 2007
Read My Lips... Part 2
I recently wrote about how to reduce hospital waiting lists.
Modern technology has come up with a new way to reduce them, as evidenced here in the SMH.
Modern technology has come up with a new way to reduce them, as evidenced here in the SMH.
3000 patients byte the dust
Lisa Carty
November 18, 2007
THE State Government has denied fudging hospital waiting list numbers, blaming the installation of a new computer for the omission of patients at two Central Coast hospitals from the latest lists.
Opposition health spokeswoman Jillian Skinner said more than 3000 people waiting for elective surgery at Gosford and Wyong hospitals had been "conveniently" dropped from the September report. If those patients had been included, the latest result would have been 56,266 people waiting up to a year for their operations, an increase on the September 2006 figure of 53,424, she said.
"They don't report this total figure at all in any press release and announcements, instead talking about a reduction in long waits [more than 12 months] which have gone down," Mrs Skinner said.
A spokeswoman for Health Minister Reba Meagher said the hospitals' figures were not on the list, published on the department website, because of the installation of a "new patient admission system".
Saturday, November 17, 2007
Clinicians Speak Out
I was recently alerted by Dr Clare Skinner (who features in this article in the AFR) as to the existence of this website, Clinicians Speak Out. To be honest, I am not 100% certain what the purpose of the website is, as it is set up like a blog, but seems to act a little like a noticeboard and a discussion forum in one. Nevertheless, the premise behind the organisation running it is straightforward - public hospitals need to be run with a clear vision and purpose. Underlying issues need to be defined and addressed, and covering up one crisis after another does not solve these issues. Attention needs to be paid to long-term planning, not short term politics.
Kudos to those brave health professionals who are willing to speak out and put their names to their concerns about the public health system. Bravo to you, and may you have a positive influence on the administration of public health. I most certainly do not have enough courage to shelve my anonymity at this time.
While the predominant focus is on public hospitals in the Sydney area (no doubt all the controversy about RNSH has brought this to the forefront, as well as the basic fact that the current NSW Health system is one of the most rundown, bureaucratic, paperwork-driven, responsibility-shedding and accountability-avoiding administrations I have every had the sad privilege of working in), every other public hospital system in Australia deserves the same attention.
So congratulations, doctors, nurses, and other health professionals at Clinicians Speak Out, may you continue to fight the good fight. I am sure that when you have some content worth reading, medical web-surfers will flock to you... in the meantime, I'll just try to boost your pageload stats because I know how good it feels. (smile)
Kudos to those brave health professionals who are willing to speak out and put their names to their concerns about the public health system. Bravo to you, and may you have a positive influence on the administration of public health. I most certainly do not have enough courage to shelve my anonymity at this time.
While the predominant focus is on public hospitals in the Sydney area (no doubt all the controversy about RNSH has brought this to the forefront, as well as the basic fact that the current NSW Health system is one of the most rundown, bureaucratic, paperwork-driven, responsibility-shedding and accountability-avoiding administrations I have every had the sad privilege of working in), every other public hospital system in Australia deserves the same attention.
So congratulations, doctors, nurses, and other health professionals at Clinicians Speak Out, may you continue to fight the good fight. I am sure that when you have some content worth reading, medical web-surfers will flock to you... in the meantime, I'll just try to boost your pageload stats because I know how good it feels. (smile)
Tuesday, November 13, 2007
Medical Students are not GPs!
Will they never learn? Kevin Rudd announced a commitment to build Family Healthcare Clinics for Defence Force members and their families. That doesn't bother me one little bit. Go for it, Kev.
This statement, however, left me frustrated that both major parties continue to fail to appreciate how the medical workforce works, and illustrates the simplistic concepts that seem to underpin major decision making amongst politicians and high-level government.
Every time the lack of doctors to staff new facilities is raised, the same response is trotted out: recruit more medical students. It sounds good. It doesn't make sense.
John Howard is not innocent of this. I have previously pointed out the problems with the Howard Government's approach to the training of doctors, but this was typical of statements at the time in February 2006:
Putting aside the qualifications that are always involved in these pronouncements ("money is being provided - but it's up to universities to implement them", "money will be invested into innovative new training schemes", "private sector training will be explored") keep in mind that many of these places will be full-fee paying (i.e. only minimally subsidised by the Government) and that they could well be occupied by overseas candidates (i.e. ones that do not contribute to the Australian Workforce).
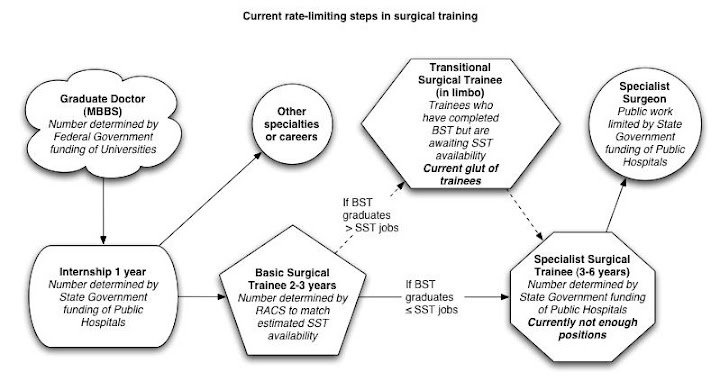
The lag time between recruiting a medical student and producing an independently practising doctor is significant: a minimum of 4-6 years before an intern is produced. Such an intern cannot staff a GP clinic. It takes another 4-6 years to do that, assuming that there are enough accredited training positions.
Depending on the specialty, such positions are limited by State Government funding of public hospitals (such as for surgery, medicine, and all of those hospital-based specialties), or by the Federal Government (via Vocationally Registered Provider Numbers for GP Trainees).
Furthermore, Provider Number and Medicare limitations means that unless a doctor completes a training program and achieves specialist recognition (including completion of GP training), they are effectively unable to service patients in the public sector. The 1996 Howard Federal Government hobbled its own ability to fill the need for GPs in its overexuberant attempt to reign in Medicare expenditure (Link 1, Link 2).
Of course, the traditional response is that training numbers are limited by Specialty College intakes, lining the pockets of specialists along the way. In reality, the Colleges go out of their way to accredit as many viable training positions as possible, but such positions can only be worthwhile if there is enough funding to treat patients and maintain throughput.
This is and will continue to be the bottleneck limiting the production of independent medical practitioners. Long-serving readers may recall that I have written about this before and while the terminology is being superceded by SET and PreSET, the basic principles remain the same.

There is a lot of talk about the impending "medical student tsunami". There is no doubt that we are turning out record numbers of medical students. Hospitals are also absorbing record numbers of Interns and RMOs, due to the enforcement of safe working hours, and the desire of these new generations of doctors to have a life outside work. These doctors are typically employed, however, in non-training positions.
Despite the best efforts of specialty colleges to approve more training positions, they are stymied by hospital and Medicare's Vocational Registration infrastructure. New graduates (and governments) are developing an expectation that they will come out of medical school and go straight into a training program, emerging as a specialist in the minimum amount of time possible.
Unless the incoming government realises that they will not be able to adequately staff these GP clinics without stealing GPs from other parts of the medical workforce, or they address all the rate-limiting steps in medical training, then we will continue to see short-sighted, short-term, sound-bite based health policy and workforce planning in Australia. We don't need politicians and political parties that make knee-jerk decisions and can't see beyond the next press conference. Unfortunately, that is all that we have to choose from.
Labor in health bid to retain personnel - The Australian
(Click to Expand)
More Doctors but not via HECS - Epoch Times
(Click to Expand)
This statement, however, left me frustrated that both major parties continue to fail to appreciate how the medical workforce works, and illustrates the simplistic concepts that seem to underpin major decision making amongst politicians and high-level government.
He denied it would be difficult to attract staff to the new medical centres, saying Labor would also invest in more medical places at universities to boost medical workforce numbers.
Labor in health bid to retain personnel - The Australian, 13 Nov 2007
Every time the lack of doctors to staff new facilities is raised, the same response is trotted out: recruit more medical students. It sounds good. It doesn't make sense.
John Howard is not innocent of this. I have previously pointed out the problems with the Howard Government's approach to the training of doctors, but this was typical of statements at the time in February 2006:
Prime Minister John Howard's February 10 announcement of a new health package at the Council of Australian Governments (COAG) meeting has drawn both criticism and praise in its addressing of the ongoing shortage of qualified doctors.
At what Prime Minister Howard described as "an unbelievably successful COAG meeting", a package of health reforms were agreed upon by state, territory and federal leaders.
In addressing the shortage of trained doctors COAG announced that there would be 25 per cent more university places made available to train new doctors but that they would be full-fee paying university places. As a part of this, incentives are to be made to increase the number of qualified doctors which includes raising the loans cap for full-fee paying medical students from $50,000 to $80,000.
More Doctors but not via HECS - Epoch Times, Feb 14 2006
Putting aside the qualifications that are always involved in these pronouncements ("money is being provided - but it's up to universities to implement them", "money will be invested into innovative new training schemes", "private sector training will be explored") keep in mind that many of these places will be full-fee paying (i.e. only minimally subsidised by the Government) and that they could well be occupied by overseas candidates (i.e. ones that do not contribute to the Australian Workforce).
The lag time between recruiting a medical student and producing an independently practising doctor is significant: a minimum of 4-6 years before an intern is produced. Such an intern cannot staff a GP clinic. It takes another 4-6 years to do that, assuming that there are enough accredited training positions.
Depending on the specialty, such positions are limited by State Government funding of public hospitals (such as for surgery, medicine, and all of those hospital-based specialties), or by the Federal Government (via Vocationally Registered Provider Numbers for GP Trainees).
Furthermore, Provider Number and Medicare limitations means that unless a doctor completes a training program and achieves specialist recognition (including completion of GP training), they are effectively unable to service patients in the public sector. The 1996 Howard Federal Government hobbled its own ability to fill the need for GPs in its overexuberant attempt to reign in Medicare expenditure (Link 1, Link 2).
Of course, the traditional response is that training numbers are limited by Specialty College intakes, lining the pockets of specialists along the way. In reality, the Colleges go out of their way to accredit as many viable training positions as possible, but such positions can only be worthwhile if there is enough funding to treat patients and maintain throughput.
This is and will continue to be the bottleneck limiting the production of independent medical practitioners. Long-serving readers may recall that I have written about this before and while the terminology is being superceded by SET and PreSET, the basic principles remain the same.
There is a lot of talk about the impending "medical student tsunami". There is no doubt that we are turning out record numbers of medical students. Hospitals are also absorbing record numbers of Interns and RMOs, due to the enforcement of safe working hours, and the desire of these new generations of doctors to have a life outside work. These doctors are typically employed, however, in non-training positions.
Despite the best efforts of specialty colleges to approve more training positions, they are stymied by hospital and Medicare's Vocational Registration infrastructure. New graduates (and governments) are developing an expectation that they will come out of medical school and go straight into a training program, emerging as a specialist in the minimum amount of time possible.
Unless the incoming government realises that they will not be able to adequately staff these GP clinics without stealing GPs from other parts of the medical workforce, or they address all the rate-limiting steps in medical training, then we will continue to see short-sighted, short-term, sound-bite based health policy and workforce planning in Australia. We don't need politicians and political parties that make knee-jerk decisions and can't see beyond the next press conference. Unfortunately, that is all that we have to choose from.
Labor in health bid to retain personnel - The Australian
(Click to Expand)
More Doctors but not via HECS - Epoch Times
(Click to Expand)
Sunday, November 11, 2007
Pay Them, and They Will Come
I came across this article in the Financial Review a few weeks ago. Unfortunately it is not online, so I have had to transcribe it manually. It raises a lot of issues - the declining status of doctors in our society, the hotch-potch of remuneration packages needed to fill gaps in medical staffing due to poor workforce planning, the loss of job satisfaction and thus the reducing amount of dedication to the job amongst new doctors.
In the same way that IT workers might flit from consulting contract to consulting contract, doctors are increasingly moving from locum position or locum position. Just as the mining boom is stealing young workers away from their apprenticeships, medical workforce gaps and locum positions steal young doctors away from their long-term training programs.
Why should you spend arduous years, giving up family time and being worked like a dog, when you can go somewhere in rural Queensland and be paid handsomely for something that you could do in your sleep?
Is There A Doctor In The House … At Any Price? - Australian Financial Review
(Click to Expand)
By the way, I can't vouch for the accuracy of the figures given at the end of this article.
In the same way that IT workers might flit from consulting contract to consulting contract, doctors are increasingly moving from locum position or locum position. Just as the mining boom is stealing young workers away from their apprenticeships, medical workforce gaps and locum positions steal young doctors away from their long-term training programs.
Why should you spend arduous years, giving up family time and being worked like a dog, when you can go somewhere in rural Queensland and be paid handsomely for something that you could do in your sleep?
Is There A Doctor In The House … At Any Price? - Australian Financial Review
(Click to Expand)
By the way, I can't vouch for the accuracy of the figures given at the end of this article.
Thursday, November 01, 2007
Read My Lips...
"Your mission, Kevin, should you decide to accept it, is to radically cut elective surgical waiting lists. Your target is to ensure that no patient is waiting beyond their waiting list category time. As usual, should you or any member of your I.M. Force be captured or killed, the secretary will disavow any knowledge of your existence. This tape will self-destruct in five seconds. Good luck, Kevin."
OK, team. This is going to be a tough one. It's going to take all of our espionage skills of misdirection, camouflage, trickery, deceipt, and social engineering to carry it off. Here is our 10 point strike plan:
The detailed operational plan can be reviewed here.
OK, team. This is going to be a tough one. It's going to take all of our espionage skills of misdirection, camouflage, trickery, deceipt, and social engineering to carry it off. Here is our 10 point strike plan:
- Spend some money to give the appearance that we are doing something that might work, even if it won't. For example, let's take, say, $100 million and give it to private hospitals, because public hospitals are crap. They can take care of a few thousand patients in the short term to buy us some time. We all know the patients will keep being added to the waiting lists faster than we can operate on them, but at least we'll look good.
- Let's ring up as many waiting patients as possible and try to convince them that they don't really need or want the operation. Even better, if they don't answer the phone or we lose their phone number, we'll say that we tried our best but have no choice but to take them off the waiting list.
- We can starve the public hospitals of funds to buy or maintain essential equipment to do operations. If the hospital is physically incapable of doing the operation we can justify delaying these operations and classify the patients as "Not Ready For Care".
- Ring up some more patients and tell them that they can have their operation at another hospital more quickly, as long as they agree to be done by a surgeon that they've never met, who won't talk to the surgeon that they have met and who may or may not be as good as the original surgeon. Then they will have to repeat all the tests again only to decide on the day of the operation that maybe they didn't need the operation in the first place. If the patient refuses we can take them off the waiting list, or say that it's the patient's fault that they are waiting.
- Fine hospitals even more for having patients waiting beyond their projected waiting time, so that hospital administration pressures the doctors to clinically reclassify patients to a less urgent category. It won't be our fault, because we'll just provide the incentive to perform better, as long as hospital executives don't tell us what they are up to.
- Redefine the waiting list categories so that the projected waiting periods are longer than before. That way it will be harder to run over time.
- Define the official date that a patient goes onto the waiting list as the date that the clerks type the form details into the computer system, not the date that the doctor filled out the form. That way we can have an extra month of physical waiting that doesn't count towards the statistics.
- Give the clerks in the waiting list office more tea breaks, and put them in a small, dark, cramped, noisy office to minimise their productivity. Therefore it will take longer before a waiting list form is physically processed, and the official waiting period will start later.
- Refuse to add patients to the waiting list unless they have their operation physically booked before entering it into the computer. That way, not only do we stay within the official target times, but we look fantastic because the patient can be physically waiting 3 months, and officially waiting one week.
- Stop these bloody doctors from putting patients onto waiting lists in the first place - let's block entry into outpatients by creating a waiting list to see a doctor, and then offer to let them see a nurse practitioner who will tell everyone that they don't need an operation. We can trust nurse practitioners to do what they are told.
The detailed operational plan can be reviewed here.
Labor pledges $600m to cut surgery waiting lists
ABC News Website
Posted Wed Oct 31, 2007 3:15pm AEDT
Updated Wed Oct 31, 2007 5:28pm AEDT
Federal Opposition Leader Kevin Rudd has unveiled details of Labor's $600 million commitment to slash elective surgery waiting lists across Australian public hospitals.
The money forms part of Labor's previously announced $2 billion health commitment.
Under the scheme, a federal Labor government would hand $100 million to the states and territories to enable public hospitals to purchase operations from private facilities.
Mr Rudd says there are 25,000 Australians on elective waiting lists who have passed the recommended time for surgery.
"The 25,000 people we are talking about, they are there now OK," he said.
"We've got an election due in November. If we win that election what I want to see is money flowing as of January 2008, out to the states and territories in order to make payments to get that 25,000 number down to zero by year's end."
But in return for the funding boost, the states would be expected to report back on their progress.
"As we speak, we will not be extending to the states a blank cheque for any of these amounts of money," Mr Rudd said.
"We will be insisting with the states that report cards be produced."
Subscribe to:
Posts (Atom)




