Will they never learn? Kevin Rudd announced a commitment to build Family Healthcare Clinics for Defence Force members and their families. That doesn't bother me one little bit. Go for it, Kev.
This statement, however, left me frustrated that both major parties continue to fail to appreciate how the medical workforce works, and illustrates the simplistic concepts that seem to underpin major decision making amongst politicians and high-level government.
He denied it would be difficult to attract staff to the new medical centres, saying Labor would also invest in more medical places at universities to boost medical workforce numbers.
Labor in health bid to retain personnel - The Australian, 13 Nov 2007
Every time the lack of doctors to staff new facilities is raised, the same response is trotted out: recruit more medical students. It sounds good. It doesn't make sense.
John Howard is not innocent of this. I have
previously pointed out the problems with the Howard Government's approach to the training of doctors, but this was typical of statements at the time in February 2006:
Prime Minister John Howard's February 10 announcement of a new health package at the Council of Australian Governments (COAG) meeting has drawn both criticism and praise in its addressing of the ongoing shortage of qualified doctors.
At what Prime Minister Howard described as "an unbelievably successful COAG meeting", a package of health reforms were agreed upon by state, territory and federal leaders.
In addressing the shortage of trained doctors COAG announced that there would be 25 per cent more university places made available to train new doctors but that they would be full-fee paying university places. As a part of this, incentives are to be made to increase the number of qualified doctors which includes raising the loans cap for full-fee paying medical students from $50,000 to $80,000.
More Doctors but not via HECS - Epoch Times, Feb 14 2006
Putting aside the qualifications that are always involved in these pronouncements (
"money is being provided - but it's up to universities to implement them", "money will be invested into innovative new training schemes", "private sector training will be explored") keep in mind that many of these places will be full-fee paying (i.e. only minimally subsidised by the Government) and that they could well be occupied by overseas candidates (i.e. ones that do not contribute to the Australian Workforce).
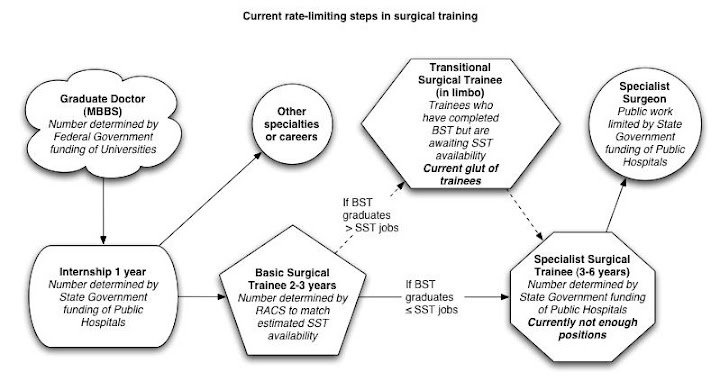
The lag time between recruiting a medical student and producing an independently practising doctor is significant: a minimum of 4-6 years before an intern is produced. Such an intern cannot staff a GP clinic. It takes another 4-6 years to do that, assuming that there are enough accredited training positions.
Depending on the specialty, such positions are limited by State Government funding of public hospitals (such as for surgery, medicine, and all of those hospital-based specialties), or by the Federal Government (via Vocationally Registered Provider Numbers for GP Trainees).
Furthermore, Provider Number and Medicare limitations means that unless a doctor completes a training program and achieves specialist recognition (including completion of GP training), they are effectively unable to service patients in the public sector. The 1996 Howard Federal Government hobbled its own ability to fill the need for GPs in its overexuberant attempt to reign in Medicare expenditure (
Link 1,
Link 2).
Of course, the traditional response is that training numbers are limited by Specialty College intakes, lining the pockets of specialists along the way. In reality, the Colleges go out of their way to accredit as many viable training positions as possible, but such positions can only be worthwhile if there is enough funding to treat patients and maintain throughput.
This is and will continue to be the bottleneck limiting the production of independent medical practitioners. Long-serving readers may recall that I have
written about this before and while the terminology is being superceded by SET and PreSET, the basic principles remain the same.

There is a lot of talk about the impending "medical student tsunami". There is no doubt that we are turning out record numbers of medical students. Hospitals are also absorbing record numbers of Interns and RMOs, due to the enforcement of safe working hours, and the desire of these new generations of doctors to have a life outside work. These doctors are typically employed, however, in non-training positions.
Despite the best efforts of specialty colleges to approve more training positions, they are stymied by hospital and Medicare's Vocational Registration infrastructure. New graduates (and governments) are developing an expectation that they will come out of medical school and go straight into a training program, emerging as a specialist in the minimum amount of time possible.
Unless the incoming government realises that they will not be able to adequately staff these GP clinics without stealing GPs from other parts of the medical workforce, or they address all the rate-limiting steps in medical training, then we will continue to see short-sighted, short-term, sound-bite based health policy and workforce planning in Australia. We don't need politicians and political parties that make knee-jerk decisions and can't see beyond the next press conference. Unfortunately, that is all that we have to choose from.
Labor in health bid to retain personnel - The Australian
(Click to Expand)Labor in health bid to retain personnel
Patricia Karvelas, Political correspondent | November 13, 2007
THE spouses and children of defence force personnel living in remote areas of Australia will have their medical and dental bills paid under a Labor plan to help retain troops.
Unveiling Labor's defence policy at the Lavarack Barracks in Townsville yesterday, Kevin Rudd committed $33.1 million for 12,000 ADF spouses and children to access free health and dental care at 12 Defence Family Healthcare Clinics.
The first two clinics will be at the Lavarack Barracks, in the marginal Liberal-held seat of Herbert, providing services for about 4000 spouses and children, and the Robertson Barracks in Darwin, which will cover 3650 spouses and children.
"This is the first time free medical and dental services are being extended to the spouses and kids of defence force personnel," Mr Rudd said.
He denied it would be difficult to attract staff to the new medical centres, saying Labor would also invest in more medical places at universities to boost medical workforce numbers.
"This policy ... is an important step forward in providing a better standard of living, a better quality of life to continue to attract people to join the defence force and to stay in the defence force," Mr Rudd said.
In 10 of the clinics, the GP will work half a day, five days a week, with a full-time nurse five days a week. A dentist and dental nurse will work five days a week.
Labor defence spokesman Joel Fitzgibbon said the health plan could be rolled out more broadly if it was successful.
"This is very much a retention initiative designed to put something on the kitchen table as defence families are considering whether to take an offer outside the ADF or stay within the ADF," he said.
Mr Rudd said that in recent years the structure of the defence force had been "torn in multiple directions".
"There had been an absence of clarity of strategic purpose, including asking our force structure to be able to maintain simultaneously hot operations in the theatres far from Australia as well as other operations near to Australia in our own immediate sphere of strategic importance here in the Southwest Pacific and Southeast Asia."
Mr Rudd said the ADF needed direction on what was expected of it in the future.
Labor was committed to all current defence projects but would ensure a new defence white paper returned discipline and strategic coherence to the Defence Capability Plan.
He said federal Labor would ensure defence was adequately funded through a commitment to at least 3 per cent real growth in spending each year.
Labor would also commission the defence white paper if it won government, with Mr Rudd asserting that defence procurement under the Howard Government had become a "rolling scandal".
"We are determined in Government to ensure that we've got the processes in place to make sure there is rational long-term planning for our equipment requirements ... which is in turn consistent with a strategic doctrine laid down in the white paper," he said.
"When you look at the long-term force structure, quite apart from immediate operations here in our own region and war-fighting operations currently occurring in various parts of the Middle East, it's very important that clarity is achieved in a new defence white paper, and that the full structure evolves from that."
(Click to Expand)More Doctors but not via HECS
By Sandra Keaton, Epoch Times, Australia Staff | February 14, 2006
Prime Minister John Howard's February 10 announcement of a new health package at the Council of Australian Governments (COAG) meeting has drawn both criticism and praise in its addressing of the ongoing shortage of qualified doctors.
At what Prime Minister Howard described as "an unbelievably successful COAG meeting", a package of health reforms were agreed upon by state, territory and federal leaders.
In addressing the shortage of trained doctors COAG announced that there would be 25 per cent more university places made available to train new doctors but that they would be full-fee paying university places. As a part of this, incentives are to be made to increase the number of qualified doctors which includes raising the loans cap for full-fee paying medical students from $50,000 to $80,000.
The Australian Industry Group (Ai Group) has said that it is confident these reforms will help assist the skills shortage currently facing the nation.
"COAG has taken important steps in helping the alleviation of skill shortages by agreeing to this raft of reforms," Ai Group chief Heather Ridout said.
Queensland Premier Peter Beattie is "delighted", as he says his state's health system will benefit – he has been lobbying for more than 300 new doctor training positions in his state.
Meanwhile Australian Medical Association President Dr Mukesh Haikerwal told the ABC that the increase in university positions will help the current shortage of Doctors. He said that it is important that enough doctors are trained but he said for that to be on a fee-paying basis is against the principles of university training and the principles of equality of access in education.
Dr Haikerwal foresees medical degrees costing students as much as $250,000.
"You know, you could have an awful lot of well-qualified people that could do medicine and do it well, having to give those places up because they can't afford this sort of money. If government is serious about getting doctors into the system and is serious about training doctors, then they need to pay for those places under the HECS system as they currently do," said Dr Haikerwal.
Doctors Reform Society President Tim Woodruff was also critical of the proposals. He said the full fee-paying medical student places were offered "to produce doctors who aren't good enough to qualify for HECS funded places".
Australian Vice Chancellors Committee CEO John Mullarvey, says he would have preferred the places to have been fully-funded by the Government.
Opposition spokeswoman Jenny Macklin saying that only government-funded university places would have helped.
"At the University of New South Wales, a medical degree costs $216,000. That leaves a huge gap for students to have to find," she said.
"We want to make sure that our doctors get there on merit not on how much their parents have got in the bank."
The Opposition also claims that Australia's university sector is being "Americanised".
The commonwealth will contribute $666 million to the health plan while another $479 million will come from the states and territories.
With AAP





No comments:
Post a Comment