"Mrs Burns?"
40 heads turn around in the outpatients waiting area as I call for the next patient. "Mrs Burns?"
A chubby elderly lady stands up with her daughter and they make their way into the windowless consulting room.
It's a fairly standard consultation. Her GP has referred this moderately obese woman in her late 50s with two episodes of colicky abdominal pain over the last six months. An ultrasound shows some small gallstones but no CBD dilatation. LFTs are normal.
It's clear that the problem is not reflux, and it has only happened twice - after Christmas dinner and a big Easter Lunch. Diagnosis: Biliary Colic.
"There's really no need to worry, Mrs Burns. The likelihood is that you will get some discomfort, maybe some diarrhoea, if you eat a very fatty meal, such as fried food. There's a very small chance that the stones could block the bile duct or gall bladder and that you might get inflammation or infection, in which case you would get quite unwell and should come to the Emergency Department. Otherwise, I would only recommend surgery if you were to develop frequent pain whenever you eat."
"Are you sure it's not cancer?" says the daughter. "My boyfriend's father's second cousin's next-door neighbour had pain like this and they found a cancer in his pancreas. He died in agony after five operations. They say it's a hidden killer."
I struggle to keep a straight face. "There is no reason to think that a cancer is there. Your mother's bowel actions are normal. Her weight is, er, stable. The blood tests are normal... at this time. I think it is just the gall stones. I'm happy to keep an eye on things, and if things were to change then I'd consider a CAT scan, but there's no reason to do that now."
"Wouldn't it be too late if she had symptoms? Why not scan her now? We don't want to end up like that bloke on the news." I sigh, silently to myself. Last week a poor chap died of a subarachnoid haemorrhage because the experienced ED physician decided that a 35 year old man with a long history of migraines didn't need yet another CT brain for yet another headache.
I could give the spiel about unnecessary radiation exposure. I could talk about blowing out the public healthcare budget and our taxes on inappropriate investigations. Or I could reach for the request slip.
"Leave the young man alone, dear. He's told us what the problem is. Don't you trust him?"
I smile to myself as I show them the door. The patient herself has let me off the hook, and highlighted the inter-generational change in "health consumer" behaviour. I cross my fingers and hope I'm right.
That was my 100th blog post. I realise that as an irregular blogger it is challenging to build up a large readership but I hope that those of you who happen to stumble upon my blog find it interesting and thought-provoking. Please keep up your comments, as that is the only way to know that somebody actually reads my blog!
Thursday, August 14, 2008
Friday, July 25, 2008
The Unwanted Child: Part 2
As a followup to my earlier post, The Unwanted Child, I thought that I would link to more recent reports in this case.
Basically the parents have been unsuccessful in their lawsuit, and I breathe a sigh of relief (as a medical professional). For more information, follow these links.
Basically the parents have been unsuccessful in their lawsuit, and I breathe a sigh of relief (as a medical professional). For more information, follow these links.
Tuesday, June 24, 2008
Heart Check? Blank Cheque! Part 2

ACA - Heart Check ConLast year, I wrote a blog entry entitled Heart Check? Blank Cheque!.
It looks like our good friend, A Current Affair, has put their "investigative skills" to the case and done a slag piece on Heart Check. Please note that I had absolutely nothing to do with this - but I don't feel the least bit sorry for them.
Clearly this piece has had more effect than my blog entry, as this Heart Check Clinic Manager reports in her blog. Hopefully it has had no involvement in her marital difficulties.
Click on the image above to see the ACA video.
Monday, June 16, 2008
Pssst! Pass it on!
A few months ago, one of my private patients took a turn for the worse. She had had a minor procedure which had gone smoothly. Unfortunately, in the several hours after the operation she developed some bleeding under the wound. I was not notified.
I returned the next day to find a tennis-ball sized haematoma, five layers of gauze and combine reinforcement, and a drain bottle that had fallen out. Multiple entries were made in the notes of the increasing haematoma, but no attempt made to contact me.
The patient was, thankfully, not upset or distressed. She was in some discomfort and agreed with me that the safest thing to do would be to return to theatre to evacuate the haematoma later that day.
Unfortunately, my secretary spent the better half of the day trying to track down an anaesthetist without success. Such is life in the private sector. Most private hospitals do not have on-call rosters, because most surgeons have direct relationships with anaesthetists that they use regularly. Unfortunately, none of mine were available at short notice, and in this situation you have to scratch around for anyone who is available and willing to come in after hours for a half-hour operation that doesn't pay very well.
After making some more phone calls myself, I managed to find a friend of a friend of a friend who was available to come in for the case. It was a simple job. A light anaesthetic, a small cut. A gentle squeeze and a few spots of diathermy. A drain tube was repositioned and the wound closed with interrupted sutures. We were all in and out of there in under an hour. The anaesthetist was jovial and friendly, and genuinely helpful. He made a point to give me his business card so that I could "Call me anytime."
 As I was writing up my notes, however, one of the anaesthetic nurses approached me. "Doctor, I'm not sure whether you know, but there's a reason Dr Anaesthetist is usually available for these cases. Apparently a few years ago he was involved when some Fentanyl went missing from the DD (Drugs of Dependency) cupboard."
As I was writing up my notes, however, one of the anaesthetic nurses approached me. "Doctor, I'm not sure whether you know, but there's a reason Dr Anaesthetist is usually available for these cases. Apparently a few years ago he was involved when some Fentanyl went missing from the DD (Drugs of Dependency) cupboard."
It turns out that the rumour was widely known - over a period of several months, the drug cupboard counts were intermittently short one or two ampoules. Not on a regular or frequent basis, but allegedly usually after a list involving this anaesthetist. It was said that he had been questioned by administration but no action taken. Since then no more drug counts had been suspicious. But the implication was clear. The anaesthetist is, or was, a drug addict.
This was a terrible allegation against an anaesthetist. It was an unproven one. No charges were laid, no disciplinary action taken. Not enough evidence existed to involve the Medical Board. All that was left was circumstance, gossip, and rumour. And a reputation that was now shattered, a career decimated.
Apparently work dried up. Lists were dropped. Phones stopped ringing. In response, this anaesthetist was forced to scrounge around for work. He had no public appointments to fall back on. He had no ICU experience to rely on. He put his name down at every private hospital in town for emergency anaesthetic work. He never said no to a case. But he had no regular lists.
I struggled with the thought of whether I should use him in the future. He seemed nice. He was competent (albeit anyone can be competent when the job is simple). The allegations were just talk and innuendo. But if they were true, how could I entrust my patients to his care? If they were false, how dare I prejudice someone based on rumour?
I never used his services again. I tell myself that it was not because of what was said - I have my regular anaesthetists, and a situation like that has not arisen since. But I feel terrible. His business card still sits in my desk drawer. I always think whether he is surviving. Occasionally we hear about an anaesthetist overdosing - I always wonder whether it is him. I have done nothing, and yet I feel guilty. That has been my secret.
I returned the next day to find a tennis-ball sized haematoma, five layers of gauze and combine reinforcement, and a drain bottle that had fallen out. Multiple entries were made in the notes of the increasing haematoma, but no attempt made to contact me.
The patient was, thankfully, not upset or distressed. She was in some discomfort and agreed with me that the safest thing to do would be to return to theatre to evacuate the haematoma later that day.
Unfortunately, my secretary spent the better half of the day trying to track down an anaesthetist without success. Such is life in the private sector. Most private hospitals do not have on-call rosters, because most surgeons have direct relationships with anaesthetists that they use regularly. Unfortunately, none of mine were available at short notice, and in this situation you have to scratch around for anyone who is available and willing to come in after hours for a half-hour operation that doesn't pay very well.
After making some more phone calls myself, I managed to find a friend of a friend of a friend who was available to come in for the case. It was a simple job. A light anaesthetic, a small cut. A gentle squeeze and a few spots of diathermy. A drain tube was repositioned and the wound closed with interrupted sutures. We were all in and out of there in under an hour. The anaesthetist was jovial and friendly, and genuinely helpful. He made a point to give me his business card so that I could "Call me anytime."
As I was writing up my notes, however, one of the anaesthetic nurses approached me. "Doctor, I'm not sure whether you know, but there's a reason Dr Anaesthetist is usually available for these cases. Apparently a few years ago he was involved when some Fentanyl went missing from the DD (Drugs of Dependency) cupboard."It turns out that the rumour was widely known - over a period of several months, the drug cupboard counts were intermittently short one or two ampoules. Not on a regular or frequent basis, but allegedly usually after a list involving this anaesthetist. It was said that he had been questioned by administration but no action taken. Since then no more drug counts had been suspicious. But the implication was clear. The anaesthetist is, or was, a drug addict.
This was a terrible allegation against an anaesthetist. It was an unproven one. No charges were laid, no disciplinary action taken. Not enough evidence existed to involve the Medical Board. All that was left was circumstance, gossip, and rumour. And a reputation that was now shattered, a career decimated.
Apparently work dried up. Lists were dropped. Phones stopped ringing. In response, this anaesthetist was forced to scrounge around for work. He had no public appointments to fall back on. He had no ICU experience to rely on. He put his name down at every private hospital in town for emergency anaesthetic work. He never said no to a case. But he had no regular lists.
I struggled with the thought of whether I should use him in the future. He seemed nice. He was competent (albeit anyone can be competent when the job is simple). The allegations were just talk and innuendo. But if they were true, how could I entrust my patients to his care? If they were false, how dare I prejudice someone based on rumour?
I never used his services again. I tell myself that it was not because of what was said - I have my regular anaesthetists, and a situation like that has not arisen since. But I feel terrible. His business card still sits in my desk drawer. I always think whether he is surviving. Occasionally we hear about an anaesthetist overdosing - I always wonder whether it is him. I have done nothing, and yet I feel guilty. That has been my secret.
Sunday, June 15, 2008
Grand Rounds (4) 38 and SurgeXperiences
Dr Crippen at NHS Blog Doctor posted this edition, and along with QuietusLeo at The Sandman, kindly included my last post on organ donation.
Please go and read them - they are fascinating links as usual.
Please go and read them - they are fascinating links as usual.
Friday, June 06, 2008
I'd like to donate my organs...
I was consenting one of my patients for a routine operation the other day (more on "informed consent" another day), when while discussing the incidence of major complications such as stroke, myocardial infarction, or death, he said to me: "Doc, if anything like that happens to me, or if it looks like I'm going to die, I'd like to donate my organs."
It struck me as rather odd that he would say that. I am sure that he had his own reasons, and I was not all that interested in why, but it made me think... would there ever be a situation where I would seriously consider referring his organs for donation? We often consider patients who present with major trauma and sudden death for organ donation, or those in ICU with head injuries and effective brain death, but patients who die as a complication of elective surgery?
The fact is, if something goes wrong while you are having elective surgery, and you end up dying, you will probably have everything possible done for you until all of your organs fail and there is not much worth harvesting. Most fatal complications of elective surgery involve cardiac failure, respiratory failure, acute renal failure. We don't often give up before at least two of these organs have failed irretrievably, and by that stage the other organs are pretty much stuffed ("stuffed" - a medical term derived from the Latin "stuffio" meaning to be beyond salvage, analogous to FUBAR).
About the only organs left are the corneas, and I have only ever successfully convinced one patient to donate them.
On the other hand, I did have a patient who died recently that had arranged to donate their body to the Anatomy School at our local university where I have previously taught. His wife had died several years ago and donated their body to research and teaching at the university, and he had made similar arrangements in advance. Even in the setting of major organ damage, this can be a useful exercise, and, in fact, is even more educational for the students when there is major pathology present. Unfortunately, permission has to be arranged for this well in advance of death for the University to be able to accept such a donation, so it is not a decision that can be made by a family after a relative dies.
Perhaps my university is a bit of a dinosaur, but we still conduct anatomical cadaveric dissections, and I believe that it is an essential learning experience, and a major tool in medical research. So the next time you are thinking of filling out your organ donation form, think also about what you want to happen to your body if it is not suitable for organ donation... perhaps donation to medical science may be a more productive way to go?
It struck me as rather odd that he would say that. I am sure that he had his own reasons, and I was not all that interested in why, but it made me think... would there ever be a situation where I would seriously consider referring his organs for donation? We often consider patients who present with major trauma and sudden death for organ donation, or those in ICU with head injuries and effective brain death, but patients who die as a complication of elective surgery?
The fact is, if something goes wrong while you are having elective surgery, and you end up dying, you will probably have everything possible done for you until all of your organs fail and there is not much worth harvesting. Most fatal complications of elective surgery involve cardiac failure, respiratory failure, acute renal failure. We don't often give up before at least two of these organs have failed irretrievably, and by that stage the other organs are pretty much stuffed ("stuffed" - a medical term derived from the Latin "stuffio" meaning to be beyond salvage, analogous to FUBAR).
About the only organs left are the corneas, and I have only ever successfully convinced one patient to donate them.
On the other hand, I did have a patient who died recently that had arranged to donate their body to the Anatomy School at our local university where I have previously taught. His wife had died several years ago and donated their body to research and teaching at the university, and he had made similar arrangements in advance. Even in the setting of major organ damage, this can be a useful exercise, and, in fact, is even more educational for the students when there is major pathology present. Unfortunately, permission has to be arranged for this well in advance of death for the University to be able to accept such a donation, so it is not a decision that can be made by a family after a relative dies.
Perhaps my university is a bit of a dinosaur, but we still conduct anatomical cadaveric dissections, and I believe that it is an essential learning experience, and a major tool in medical research. So the next time you are thinking of filling out your organ donation form, think also about what you want to happen to your body if it is not suitable for organ donation... perhaps donation to medical science may be a more productive way to go?
Monday, May 19, 2008
SurgeXperiences Carnival 122
It’s been eye-opening to read submissions from all over the medical blogosphere this fortnight. This is the first blog carnival I have hosted, and I now appreciate the amount of effort that previous hosts have put into it.
A few weeks ago, a young man presented with a chicken bone lodged transversely in his distal rectum. After the ED registrar and consultant had spent over an hour trying to remove it, I thought it would be easiest to cut it in half. Dr Wes felt that he had a similar epiphany in MacGyver Moments in Medicine.
I’m not sure whether this qualifies as pornography or a fetish post, but Make Mine Trauma at IntraopOrate describes in Oh Say Can You See her secret fantasy of seeing her internal organs. Hey, anything that gets your rocks off, baby. ;-)
MB Herrera at Life, Money & Development describes in Natural Recipe for a Healthy Prostate some Level 6 evidence for relieving BPH. Personally, I think it is the result of too much masturbation... but you can't stop human nature, can you?
When I first read Øystein’s blog I thought: “This guy has too much time on his hands.” I quickly realised that he is not just a voyeur, but films operations for a living. His submission was "Filming surgery with camcorders". My tip - never let a sound recordist into your theatre, and if they do, insist that they remove that hairy dog from their microphone, unless you are happy for your patient to have their wound infected with bizarre and rare bacteria or fungi.
In a post reminiscent of poor Otto in Helen Palmer's "A Fish Out Of Water", TherapyDoc submitted "The End Stage" where she seems to have reached a zen moment with her fishy charge.
Bongi almost didn't make it in with Surgical Ego because he didn't flatter me enough, but I felt that I had to prove him wrong. Therefore I'm also listing his other submission No Wining about the trials and tribulations of being berated in a unit meeting. Don't worry, I once had the same experience (and criticism) after doing a trauma thoracotomy in ED. May I refer you to this article? It has helped me enormously.
Dr Deb writes about a man who apparently underwent hand surgery without any anaesthesia, placing himself into a trance only. Honestly, I didn’t find this very interesting. It left me feeling rather numb.
Suthacha_Xiang Mei writes about her first surgical rotation. It's always good to see some enthusiasm in our medical students, locally and globally.
Thanks everyone for a great range of submissions, and I wish you all the best in your blogging lives – and please keep reading my blog, too! Please keep reading SurgeXperiences and the next carnival will be hosted in a fortnight at The Sandman. Post submissions here.
A few weeks ago, a young man presented with a chicken bone lodged transversely in his distal rectum. After the ED registrar and consultant had spent over an hour trying to remove it, I thought it would be easiest to cut it in half. Dr Wes felt that he had a similar epiphany in MacGyver Moments in Medicine.
I’m not sure whether this qualifies as pornography or a fetish post, but Make Mine Trauma at IntraopOrate describes in Oh Say Can You See her secret fantasy of seeing her internal organs. Hey, anything that gets your rocks off, baby. ;-)
MB Herrera at Life, Money & Development describes in Natural Recipe for a Healthy Prostate some Level 6 evidence for relieving BPH. Personally, I think it is the result of too much masturbation... but you can't stop human nature, can you?
When I first read Øystein’s blog I thought: “This guy has too much time on his hands.” I quickly realised that he is not just a voyeur, but films operations for a living. His submission was "Filming surgery with camcorders". My tip - never let a sound recordist into your theatre, and if they do, insist that they remove that hairy dog from their microphone, unless you are happy for your patient to have their wound infected with bizarre and rare bacteria or fungi.
In a post reminiscent of poor Otto in Helen Palmer's "A Fish Out Of Water", TherapyDoc submitted "The End Stage" where she seems to have reached a zen moment with her fishy charge.
Bongi almost didn't make it in with Surgical Ego because he didn't flatter me enough, but I felt that I had to prove him wrong. Therefore I'm also listing his other submission No Wining about the trials and tribulations of being berated in a unit meeting. Don't worry, I once had the same experience (and criticism) after doing a trauma thoracotomy in ED. May I refer you to this article? It has helped me enormously.
Dr Deb writes about a man who apparently underwent hand surgery without any anaesthesia, placing himself into a trance only. Honestly, I didn’t find this very interesting. It left me feeling rather numb.
Suthacha_Xiang Mei writes about her first surgical rotation. It's always good to see some enthusiasm in our medical students, locally and globally.
Thanks everyone for a great range of submissions, and I wish you all the best in your blogging lives – and please keep reading my blog, too! Please keep reading SurgeXperiences and the next carnival will be hosted in a fortnight at The Sandman. Post submissions here.
Sunday, May 11, 2008
SurgeXperiences Carnival Submissions
As I am hosting the next SurgeXperiences Blog Carnival on May 25, I guess I better read some blog entries.
I have no rules - just go ahead and make your submission and then I'll read them. I'm not one to post everything that gets submitted - but don't take any omission as a personal rejection... It's most likely I just didn't get around to reading it!
I have no rules - just go ahead and make your submission and then I'll read them. I'm not one to post everything that gets submitted - but don't take any omission as a personal rejection... It's most likely I just didn't get around to reading it!
Thursday, May 08, 2008
Storm Clouds Gather
Mrs Hodge walks in with her wheelie frame. She is not happy. Neither is her daughter.
"I'm sorry about the wait," I say as I usher them into the cramped, drab Outpatients cubicle. "As you can see, we have been very busy and are a bit behind".
"So you should be," she snaps. "I've been out there for an hour and a half. This is pathetic. You better fix me or I'm walking out of here now."
I already get the feeling that this will be a difficult consultation, as both women scowl at me.
"So could you tell me what the problem is, Mrs Hodge?"
"You tell me, you're the doctor!"
I scan the GP letter again.
Oh dear. I could think of quite a few reasons why the GP had no referring details - but the real reason was becoming quite obvious.
"Unfortunately the GP has not given me much information. I'm relying on you to give me some idea. What have you noticed that has been wrong recently?"
"I have stomach problems."
"What kind of stomach problems?" I enquire - now we are getting somewhere.
"It hurts sometimes. Some times I feel sick."
"How long has this been going on for?"
"A while."
Silence.
"Well, are we talking a few days, a few months, years?"
"Years."
"5, 10, 20? All your life?"
"At least 5 years." The scowl has not moved since the consultation started. I know things are going badly when I degenerate into closed questioning within the first 30 seconds.
"So less than 10?"
"That's what I said. At least 5." The patient is getting agitated. "Aren't you listening? I said 5 years. What kind of doctor are you?"
"OK, where do you feel this discomfort? Does it happen at any specific time? After meals? Does it last long? What do you do to make it better? Is it worse when you lie down? Do you ever vomit or feel like vomiting?" There is no way that open questioning will do any good here.
"Sometimes in my chest, sometimes in my tummy. Sometimes it happens with food. Sometimes I just get it. It goes away after a while. Usually I feel sick but I don't vomit."
The consultation is stalling, so I move the patient into the examination bay, and find some mild right upper quadrant tenderness, and some epigastric tenderness. My money is on gallstones, but there is also a small umbilical hernia.
"So when you get this discomfort, is it mainly in your chest or in your tummy? Can you point to where it is? Have you ever had pain in your shoulder?"
"Haven't we been here before?" Her daughter interjects, as the patient starts waving her hand around her torso. "What kind of question is that? Don't you listen? Why are you asking about her chest and shoulder? She said it was her stomach." I start wishing I hadn't invited her in.
"Firstly, I need to ask these questions because it could be a number of problems. Clearly your situation is not straightforward, and I'm trying to establish what the main issue is. What bothers you most: stomach pain, or nausea?"
It's the patient's turn to chime in. "I told you it was my stomach. What's wrong with you? I came here because of my stomach - 6 years of medicine and you think you're all high and mighty. Why ask me what the problem is? I don't have a medical degree. It's people like you that really disgust me." She all but spits on the floor.
"I'm here to try to work out what is going on. Obviously you don't approve of what I am doing, and we aren't making a great deal of progress with your symptoms." It has already taken 20 minutes of tense negotiation to get the information that I have. Like drawing blood from a stone. "I have other patients waiting, but at the moment I'm prepared to offer you an ultrasound and some antacid tablets to start with, and an ECG. I can see you in 2 weeks with the results or, if you don't wish to see me, you can make an appointment to see one of the other surgeons at the hospital."
"Hang on a minute." Storm clouds start gathering as I hear thunder in the background. "I didn't say anything about not wanting to see you. You're just trying to get rid of me. Go on, close my file, you sick bastard."
"Mrs Hodge, it's clear that this consultation is not working for either of us. I am still prepared to organise your tests and send a letter to your GP, but clearly you are too agitated to continue. If you wish to come back we can discuss the results in two weeks."
"You can take your tests and shove it up your arse. I'm leaving. Where do you get off treating me like a dog?" She and her daughter storm out of the cubicle. I can hear them loudly complaining outside as I pick up the telephone and let the Patient Liaison Officer know that she will be meeting some very upset people soon.
"I'm sorry about the wait," I say as I usher them into the cramped, drab Outpatients cubicle. "As you can see, we have been very busy and are a bit behind".
"So you should be," she snaps. "I've been out there for an hour and a half. This is pathetic. You better fix me or I'm walking out of here now."
I already get the feeling that this will be a difficult consultation, as both women scowl at me.
"So could you tell me what the problem is, Mrs Hodge?"
"You tell me, you're the doctor!"
I scan the GP letter again.
Dear Dr Sheepish:
Thankyou for reviewing this 68 year old woman. Please assess, investigate and manage as appropriate.
Kind regards,
Dr GP.
Oh dear. I could think of quite a few reasons why the GP had no referring details - but the real reason was becoming quite obvious.
"Unfortunately the GP has not given me much information. I'm relying on you to give me some idea. What have you noticed that has been wrong recently?"
"I have stomach problems."
"What kind of stomach problems?" I enquire - now we are getting somewhere.
"It hurts sometimes. Some times I feel sick."
"How long has this been going on for?"
"A while."
Silence.
"Well, are we talking a few days, a few months, years?"
"Years."
"5, 10, 20? All your life?"
"At least 5 years." The scowl has not moved since the consultation started. I know things are going badly when I degenerate into closed questioning within the first 30 seconds.
"So less than 10?"
"That's what I said. At least 5." The patient is getting agitated. "Aren't you listening? I said 5 years. What kind of doctor are you?"
"OK, where do you feel this discomfort? Does it happen at any specific time? After meals? Does it last long? What do you do to make it better? Is it worse when you lie down? Do you ever vomit or feel like vomiting?" There is no way that open questioning will do any good here.
"Sometimes in my chest, sometimes in my tummy. Sometimes it happens with food. Sometimes I just get it. It goes away after a while. Usually I feel sick but I don't vomit."
The consultation is stalling, so I move the patient into the examination bay, and find some mild right upper quadrant tenderness, and some epigastric tenderness. My money is on gallstones, but there is also a small umbilical hernia.
"So when you get this discomfort, is it mainly in your chest or in your tummy? Can you point to where it is? Have you ever had pain in your shoulder?"
"Haven't we been here before?" Her daughter interjects, as the patient starts waving her hand around her torso. "What kind of question is that? Don't you listen? Why are you asking about her chest and shoulder? She said it was her stomach." I start wishing I hadn't invited her in.
"Firstly, I need to ask these questions because it could be a number of problems. Clearly your situation is not straightforward, and I'm trying to establish what the main issue is. What bothers you most: stomach pain, or nausea?"
It's the patient's turn to chime in. "I told you it was my stomach. What's wrong with you? I came here because of my stomach - 6 years of medicine and you think you're all high and mighty. Why ask me what the problem is? I don't have a medical degree. It's people like you that really disgust me." She all but spits on the floor.
"I'm here to try to work out what is going on. Obviously you don't approve of what I am doing, and we aren't making a great deal of progress with your symptoms." It has already taken 20 minutes of tense negotiation to get the information that I have. Like drawing blood from a stone. "I have other patients waiting, but at the moment I'm prepared to offer you an ultrasound and some antacid tablets to start with, and an ECG. I can see you in 2 weeks with the results or, if you don't wish to see me, you can make an appointment to see one of the other surgeons at the hospital."
"Hang on a minute." Storm clouds start gathering as I hear thunder in the background. "I didn't say anything about not wanting to see you. You're just trying to get rid of me. Go on, close my file, you sick bastard."
"Mrs Hodge, it's clear that this consultation is not working for either of us. I am still prepared to organise your tests and send a letter to your GP, but clearly you are too agitated to continue. If you wish to come back we can discuss the results in two weeks."
"You can take your tests and shove it up your arse. I'm leaving. Where do you get off treating me like a dog?" She and her daughter storm out of the cubicle. I can hear them loudly complaining outside as I pick up the telephone and let the Patient Liaison Officer know that she will be meeting some very upset people soon.
Tuesday, April 22, 2008
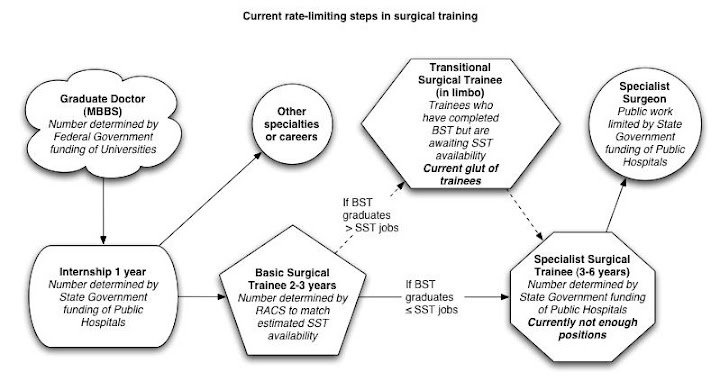
Nurses Need Hospital Training
Does this sound strangely familiar?
Firstly, this is what happens when you take training out of the hospital system for nurses - when they realise it is a good thing, they can't get back in.
Secondly, student nurses could get plenty of clinical training on-the-job if they returned to working junior nursing positions, but that sort of makes universities redundant - what would you do with all the clinical educators and nursing preceptors?
Lastly, this sounds like exactly the same issues that postgraduate doctors face in getting their specialist experience! Doesn't anyone ever learn?
NB This diagram is a little out of date but nonetheless relevant.

Hospital bottleneck stymies nurse plan
Siobhain Ryan | April 20, 2008 - The Australian
GOVERNMENT needs to put the brakes on plans on massively boost nursing numbers until they solve the worst shortage in hospital training places the profession has seen, John Daly, Chair of the Council of Deans of Nursing and Midwifery (Australia and New Zealand), said.
Professor Daly, speaking on the sidelines of the 2020 Summit in Canberra, said in some states such as New South Wales, nursing undergraduates were already unable to do the hours of practical clinical training in hospitals required to complete their courses.
"This is the worst we’ve seen it, and it’s not just in NSW. The Deans of Nursing and Midwifery are saying it’s a problem across the country," he said.
The Rudd Government’s health policy relies heavily on its promise to ramp up the number of nurses and other health workers, announcing last month it would train up to 50,000 new frontline health professionals.
Pre-election, it also committed $81 million towards putting 9,250 extra nurses into Australia’s hospital system.
But Professor Daly said governments had to address existing bottlenecks in supervised clinical hours in hospitals, and expand training opportunities for undergraduates in GP practices and community health, if it was not to exacerbate the crisis.
"Let’s be very cautious before we rush to increase them any further before we resolve this clinical training problem," he said.
Firstly, this is what happens when you take training out of the hospital system for nurses - when they realise it is a good thing, they can't get back in.
Secondly, student nurses could get plenty of clinical training on-the-job if they returned to working junior nursing positions, but that sort of makes universities redundant - what would you do with all the clinical educators and nursing preceptors?
Lastly, this sounds like exactly the same issues that postgraduate doctors face in getting their specialist experience! Doesn't anyone ever learn?
NB This diagram is a little out of date but nonetheless relevant.
Sunday, April 20, 2008
Ward Fashion
Paging Dr has had some discussion on fashion amongst medical students and junior doctors. In Australia, we don't generally have the advantage of covering everything with a white lab coat. I'm no fashionista, and I recognise that there is a great deal of variety in how people choose to dress.From a practical standpoint, These are my tips for fashion in the clinical environment:
- Wear something easy to change. Especially if you are going to enter theatre, you don't want to have to spend forever getting changed.
- Wear something stain resistant. Blood, pus and goo are regular staples on the wards. You want something that you can wash, or dry-clean without breaking your budget.
- Wear something comfortable, or which will become comfortable. You will be working long days, and do not want to have to keep taking things on and off all the time. This is especially true for footwear. Not many of us have a luxury of an office or a locker. Having said that, if you get one, hold onto it for dear life.
- Avoid short skirts or low necklines. Unlike TV shows, hospitals are not a pick-up venue. You are here for work or study, and there are no janitor's closets for you to have a quickie in. Apart from what your colleagues might or might not think, you also have patients to think about. One of my interns once complained that she could not insert any male IDCs, because they would always have an erection when she came to do it. I had to explain that showing your cleavage every time you bend over might not be helping. Also remember that geriatric wards are often full of disinhibited old men. Nurses learn very quickly not to lean over in short skirts. You should too.
- Do not dress more formally than your registrar or consultant. Especially if you are mature-age, you do not want patients to think you are the boss. It is embarassing for you, the consultant, and the patient. On the other hand, if your consultant likes to prance around in leather jackets or looks like a frumpy old housewife, then anything goes.
- Avoid jewellery. Bling does not make you look more professional. Bling makes it difficult to wash your hands or to wear gloves. Bling has lots of crevices where blood is hard to clean out. Bling has a tendency to disappear.
Don't worry if you can't remember the rules. Sooner or later you will work them out, but there might be a few unpleasant experiences along the way.
Friday, April 18, 2008
SurgeXperiences 19
As every new inbound link is precious to me (mainly because I don't have that many) I have agreed to host one of these Blog Carnival thingies in the next few weeks. This is somewhat of a problem since I tend to just write what I think, and don't go around reading other people's blogs all the time unless there is something specific that catches my eye. Does that make me a hypocrite?
In any case, I suppose the fact that I am hosting a Blog Carnival means I am obliged to start promoting it. And I will have to read all these submissions.
So, here you go: SurgeXperiences Issue 19 is out at Marianas Eye. You can view it here.
In any case, I suppose the fact that I am hosting a Blog Carnival means I am obliged to start promoting it. And I will have to read all these submissions.
So, here you go: SurgeXperiences Issue 19 is out at Marianas Eye. You can view it here.
Sunday, April 13, 2008
All Gloved Up and Nowhere To Go
 My experience is that about one in 20 examination gloves (not to be confused with surgical gloves) have a fault of some sort - breaking while being put on, unexpected size discrepancy, holes present already in the glove, deformed glove or adherent to another glove.
My experience is that about one in 20 examination gloves (not to be confused with surgical gloves) have a fault of some sort - breaking while being put on, unexpected size discrepancy, holes present already in the glove, deformed glove or adherent to another glove.I must admit, however, that I am not a big glove wearer. Cringe if you will, but I do not wear gloves to examine groins, scrota, or feet. I only go to the trouble of donning them if there is an ulcer, wound, pus, or (potential) intertrigo (commonly known as skin-fold porridge). I am, however, an avid hand washer and user of alcoholic hand rubs.
I also do not wear gloves when putting in IVs or taking blood. A poorly fitting examination glove is completely useless to me as protection against a needlestick injury. If non-sterile surgical gloves were cheaply available I'd consider wearing them - but poor quality examination gloves only make my job more difficult and dangerous.
From The Australian - Examination gloves fail lab testing
(Click to Expand)
Thursday, March 27, 2008
Listen to me...

Every now and again I see someone who is interested in buying an electronic stethoscope. I think it's great for people with hearing impediments. But I think it should stop there. If you keep going, then what is the difference between a stethoscope and a portable ultrasound or echo machine?
Patient: "Hi, I'm booked for a Stethoscopy?"
Receptionist: "Yes, Mr Patient. Please take a seat. The Cardiologist will be with you soon."
...
Cardiologist: "Hi, Mr Patient. Please come in, and remove your shirt. Today we'll be doing an auscultation."
Patient: "That's a fancy piece of equipment there, doctor."
Cardiologist: "Yes, it's worth a fortune and has revolutionised how we charge, um, I mean, examine patients these days."
... Cardiologist performs auscultation and 45 minutes later ...
Cardiologist: "Thanks Mr Patient, that's the end of the auscultatory investigation. We'll analyse your heart sounds on the computer this evening and send the report to your GP."
Receptionist: "That will be $150 Mr Patient. Please sign this form and Medicare will reimburse you... um, nothing."
Cardiologist (in his office): "Mwaa ha ha ha ha ha ha! Just to think that would take 2 minutes with a regular stethoscope and I'd be making nothing on it! God thank the genius who turned auscultation into a separate complex investigation! Mwaa ha ha ha ha ha!"
Wednesday, March 12, 2008
I don't care...
This article in Academic Medicine recently caught my eye, observing that US medical students have a declining level of empathy for their patients during the course of their studies.
Let me summarise this briefly. Conclusions:
I'm no rocket scientist, but I take issue with the belief that Vicarious Empathy is a good thing. Getting teary when discussing the risks of intraoperative death during elective surgery is not a good thing. Getting butterflies when a patient tells me about their grandchild with a congenital heard disorder distracts me from looking after the patient. But then again I'm a surgeon... who am I to comment?
March 2008, 83:3
Fulltext | PDF (82 K)
Is There Hardening of the Heart During Medical School?
Physician-Patient Relationship
Academic Medicine. 83(3):244-249, March 2008.
Newton, Bruce W. PhD; Barber, Laurie MD; Clardy, James MD; Cleveland, Elton MD; O'Sullivan, Patricia EdD
Abstract:
Purpose: To determine whether vicarious empathy (i.e., to have a visceral empathic response, versus role-playing empathy) decreases, and whether students choosing specialties with greater patient contact maintain vicarious empathy better than do students choosing specialties with less patient contact.
Method: The Balanced Emotional Empathy Scale was administered at the beginning of each academic year at the University of Arkansas for Medical Sciences for four classes, 2001-2004. Students also reported their gender and specialty choice. Specialty choice was classified as core (internal medicine, family medicine, obstetrics-gynecology, pediatrics, and psychiatry) or noncore (all other specialties).
Results: Vicarious empathy significantly decreased during medical education (P < .001), especially after the first and third years. Students choosing core careers had higher empathy than did those choosing noncore careers. Men choosing core careers initially had empathy exceeding population norms, but their empathy fell to be comparable with that of norms by the end of their third year. The empathy of men choosing noncore careers was comparable with that of norms. Women choosing core careers had empathy scores comparable with those of norms, but the scores of women choosing noncore careers fell below those of the norms by their second year.
Conclusions: The findings suggest that undergraduate medical education may be a major determinant differentially affecting the vicarious empathy of students on the basis of gender and/or specialty choice. The greatest impact occurred in men who chose noncore specialties. The significant decrease in vicarious empathy is of concern, because empathy is crucial for a successful physician-patient relationship.
(C) 2008 Association of American Medical Colleges
Let me summarise this briefly. Conclusions:
- "Vicarious empathy" is the empathic response you can't control, the "gut feeling".
- "Imaginative empathy" is something that can be acquired - "What if I were in their shoes?"
- Empathy = Good (a generalisation)
- The more empathic you were before you started medicine the more likely you would be empathic at the end.
- Everybody loses vicarious empathy during the course of their degree.
- If you chose to specialise into surgery pathology or radiology you were (likely to be) less empathic.
I'm no rocket scientist, but I take issue with the belief that Vicarious Empathy is a good thing. Getting teary when discussing the risks of intraoperative death during elective surgery is not a good thing. Getting butterflies when a patient tells me about their grandchild with a congenital heard disorder distracts me from looking after the patient. But then again I'm a surgeon... who am I to comment?
Wednesday, February 20, 2008
Technical Hitch
Apologies to those who have trouble expanding collapsed articles for reading. The relevant piece of HTML/Javascript magickery has been repaired.
Tuesday, February 19, 2008
A Traumatic Experience
For those who are unaware, there is a surgeon in Melbourne who has been the subject of a number of accusations leading to his suspension, amongst them that he is difficult to work with (or for), that he performs unnecessary operative procedures on serious trauma patients, and that he has been engaging in improper billing practices. These allegations are currently being hotly debated in the press and also the subject of a Supreme Court action.
I do not pass judgement about his character, surgical decision-making, or skill.
These two articles, however, have caught my attention:
TAC probes its links to hospitals - The Age
(Click to Expand)
Surgeons' billing questioned by secret TAC audit - The Age
(Click to Expand)
For those not familiar with the TAC (or Victorian Transport Accident Commission) its role is to act as a defacto private health insurer for those people sustaining personal injuries as a result of traffic accidents in Victoria, Australia - similar to the Motor Accidents Authority of NSW. It is funded by way of compulsory insurance premiums paid by all motor vehicle registrants in that state (currently around $300-$400 a year for a standard passenger vehicle).
From its website:
The TAC is fairly flexible on what it pays out - it was established to cover all the long-term out-of-pocket and accessory costs of a serious traffic injury, such as those incurred by someone with a major spinal or head injury. Often these are costs which are not well funded through Medicare, or are often not covered under Private Health Insurance. It is analogous in function to the various WorkCover or WorkSafe schemes - and as such can be the subject of similar client (patient or claimant) abuse.
The way that it operates is very similar to that of a Private Health Insurer with fantastic "extras" cover - physiotherapy, long-term rehabilitation, dental care, transport costs, specialised equipment, carer's costs etc. In-hospital costs are paid for treatment in public and private hospitals. For public hospitals, these rates are agreed upon between the TAC and the Victorian Department of Human Services. Generally the TAC has to give written or telephone approval for anything outside of an emergency situation.
Obviously, public hospitals love TAC patients the same way that they love privately insured patients - it is money in the bank for them.
The TAC also has set fees for surgery and consultations which it will pay to doctors who engage in private practice, or have the right of private practice in a public hospital (i.e. Consultant Staff Specialists or VMOs). Where these fees are not paid directly to the doctor it is common that they are paid into a Private Practice Fund, "Dillon Fund", or some other trust fund often administered by the hospital.
The concerns raised in these two articles relate to firstly, whether Professor Kossman or his colleagues were entitled to TAC payments for services rendered by them or on their behalf, and secondly whether the TAC should be paying for services for which patients would be entitled to care in the public hospital system already.
These strike to the heart of several deeper issues:
1. Does the TAC require specialists to render services directly to the patient, or is it acceptable to (directly or indirectly) supervise or delegate this treatment to a junior or assistant?
There does not seem to be any specific rule about this, and it is common for orthopaedic registrars to perform procedures on TAC patients with the bill still going to the TAC. This is in contradiction to the general practice whereby privately insured patients should be directly operated upon by their chosen specialist - as this is a condition of Medicare funding their portion of the patient's medical fee.
Does the TAC draw upon Medicare to pay the bulk of these fees in the same way as a private health insurer? If not, then what rules exist to say that the operating surgeon or consulting physician must be the one who personally rendered the service?
Clearly The Alfred Hospital has been claiming TAC fees on behalf of Professor Kossman and his colleagues. Presumably these fees were paid into a pooled private practice fund of some sort. Was some arrangement as part of his employment contract reached whereby Professor Kossman received a greater proportion of these payments than other doctors? Does The Alfred have the right to use TAC or private insurance payments to "sweeten the deal"? Did Professor Kossman raise the profile of some questionable practices as a result of his high operative load?
As for the issue of demonstrating that consultations occurred - this relates to the perennial issue of medical record-keeping. Nobody I know is a perfect record keeper. I most certainly am not. I try to make a short entry every time I see someone in private, but I am not infallible. Generally I rely on my junior staff to do that in public - and I would not be surprised if they were to omit the fact of my attendance in the interests of brevity. It is not the least surprising that some consultations were undocumented.
2. Should the TAC pay for the costs incurred by a public hospital for covered patients?
If the TAC did not exist (such as in Queensland) the Victorian State Government would still have to pay for the care of these patients in the public hospital system, but there is no doubt that their out-of-hospital care would be cost-shifted to the Federal Government and also be of significantly poorer quality. It would, however, be cheaper.
However, part of the reason for the TAC's payment scheme is to allow patients to exit the public hospital system and be treated in private hospitals. This benefits the public hospital system by reducing demand on resources, and also encourages the development of efficient specialist treatment centres for people with severe traffic-related injuries. A number of private rehabilitation centres specialise in TAC-related work. The Austin Hospital's Spinal Injury Unit is constantly filled with TAC-funded patients. And Melbourne's Alfred Hospital is presumably an excellent first-line major trauma centre, and therefore handles large numbers of TAC-insured patients.
No doubt having specialised centres giving excellent care may drive down the short-term costs (by way of volume and system efficiency savings) and long-term costs (by way of giving the best clinical and functional result, thereby leading to fewer ongoing care costs) for these groups of patients, but it also means that these centres will strive to provide the best care available to them by engaging to treatments and investigations which are costly in the short term and potentially less rewarding in the long term... effectively having a decreasing "bang for the buck" to put it crudely.
Perhaps these are issues which raise more questions than answers, but I believe that they deserve more attention than what is portrayed in the news and general media.
Background News Articles from The Age:
I do not pass judgement about his character, surgical decision-making, or skill.
These two articles, however, have caught my attention:
TAC probes its links to hospitals - The Age
(Click to Expand)
Surgeons' billing questioned by secret TAC audit - The Age
(Click to Expand)
For those not familiar with the TAC (or Victorian Transport Accident Commission) its role is to act as a defacto private health insurer for those people sustaining personal injuries as a result of traffic accidents in Victoria, Australia - similar to the Motor Accidents Authority of NSW. It is funded by way of compulsory insurance premiums paid by all motor vehicle registrants in that state (currently around $300-$400 a year for a standard passenger vehicle).
From its website:
The TAC is a Victorian Government-owned organisation set up in 1986.
Its role is to pay for treatment and benefits for people injured in transport accidents. It is also involved in promoting road safety in Victoria and in improving Victoria's trauma system.
Funding used by the TAC to perform these functions comes from payments made by Victorian motorists when they register their vehicles each year with VicRoads.
The TAC is a "no-fault" scheme. This means that medical benefits will be paid to an injured person - regardless of who caused the accident.
Legislation guides the TAC in the types of benefits it can pay and any conditions that apply. This legislation is called the Transport Accident Act 1986.
To ensure it remains a long-term compensation scheme, the TAC uses its funds fairly and responsibly. This ensures the TAC is able to meet the needs of seriously injured people who need lifetime care.
The TAC is fairly flexible on what it pays out - it was established to cover all the long-term out-of-pocket and accessory costs of a serious traffic injury, such as those incurred by someone with a major spinal or head injury. Often these are costs which are not well funded through Medicare, or are often not covered under Private Health Insurance. It is analogous in function to the various WorkCover or WorkSafe schemes - and as such can be the subject of similar client (patient or claimant) abuse.
The way that it operates is very similar to that of a Private Health Insurer with fantastic "extras" cover - physiotherapy, long-term rehabilitation, dental care, transport costs, specialised equipment, carer's costs etc. In-hospital costs are paid for treatment in public and private hospitals. For public hospitals, these rates are agreed upon between the TAC and the Victorian Department of Human Services. Generally the TAC has to give written or telephone approval for anything outside of an emergency situation.
Obviously, public hospitals love TAC patients the same way that they love privately insured patients - it is money in the bank for them.
The TAC also has set fees for surgery and consultations which it will pay to doctors who engage in private practice, or have the right of private practice in a public hospital (i.e. Consultant Staff Specialists or VMOs). Where these fees are not paid directly to the doctor it is common that they are paid into a Private Practice Fund, "Dillon Fund", or some other trust fund often administered by the hospital.
The concerns raised in these two articles relate to firstly, whether Professor Kossman or his colleagues were entitled to TAC payments for services rendered by them or on their behalf, and secondly whether the TAC should be paying for services for which patients would be entitled to care in the public hospital system already.
These strike to the heart of several deeper issues:
1. Does the TAC require specialists to render services directly to the patient, or is it acceptable to (directly or indirectly) supervise or delegate this treatment to a junior or assistant?
There does not seem to be any specific rule about this, and it is common for orthopaedic registrars to perform procedures on TAC patients with the bill still going to the TAC. This is in contradiction to the general practice whereby privately insured patients should be directly operated upon by their chosen specialist - as this is a condition of Medicare funding their portion of the patient's medical fee.
Does the TAC draw upon Medicare to pay the bulk of these fees in the same way as a private health insurer? If not, then what rules exist to say that the operating surgeon or consulting physician must be the one who personally rendered the service?
Clearly The Alfred Hospital has been claiming TAC fees on behalf of Professor Kossman and his colleagues. Presumably these fees were paid into a pooled private practice fund of some sort. Was some arrangement as part of his employment contract reached whereby Professor Kossman received a greater proportion of these payments than other doctors? Does The Alfred have the right to use TAC or private insurance payments to "sweeten the deal"? Did Professor Kossman raise the profile of some questionable practices as a result of his high operative load?
As for the issue of demonstrating that consultations occurred - this relates to the perennial issue of medical record-keeping. Nobody I know is a perfect record keeper. I most certainly am not. I try to make a short entry every time I see someone in private, but I am not infallible. Generally I rely on my junior staff to do that in public - and I would not be surprised if they were to omit the fact of my attendance in the interests of brevity. It is not the least surprising that some consultations were undocumented.
2. Should the TAC pay for the costs incurred by a public hospital for covered patients?
If the TAC did not exist (such as in Queensland) the Victorian State Government would still have to pay for the care of these patients in the public hospital system, but there is no doubt that their out-of-hospital care would be cost-shifted to the Federal Government and also be of significantly poorer quality. It would, however, be cheaper.
However, part of the reason for the TAC's payment scheme is to allow patients to exit the public hospital system and be treated in private hospitals. This benefits the public hospital system by reducing demand on resources, and also encourages the development of efficient specialist treatment centres for people with severe traffic-related injuries. A number of private rehabilitation centres specialise in TAC-related work. The Austin Hospital's Spinal Injury Unit is constantly filled with TAC-funded patients. And Melbourne's Alfred Hospital is presumably an excellent first-line major trauma centre, and therefore handles large numbers of TAC-insured patients.
No doubt having specialised centres giving excellent care may drive down the short-term costs (by way of volume and system efficiency savings) and long-term costs (by way of giving the best clinical and functional result, thereby leading to fewer ongoing care costs) for these groups of patients, but it also means that these centres will strive to provide the best care available to them by engaging to treatments and investigations which are costly in the short term and potentially less rewarding in the long term... effectively having a decreasing "bang for the buck" to put it crudely.
Perhaps these are issues which raise more questions than answers, but I believe that they deserve more attention than what is portrayed in the news and general media.
Background News Articles from The Age:
Sunday, February 17, 2008
Walking backwards, slowly.
I have been following, on and off, a thread on Paging Dr about how to "Survive First Year". After three pages of posts it is a bit muddled about the first year of what, but all the talk about work-life balance has raised the hairs on the back of my neck.
Now don't get me wrong, I am not against doctors having a social life and being able to wind down away from work. Heaven forbid, my family would be very unhappy if I completely ignored them to work all day and all night.
But this concept that doctors (and medical students) are entitled to a fun and enjoyable experience during their work or study irks me. Medical school is meant to get you trained up as a decent doctor... but it just so happens that all the students want it to be fun and enjoyable. Being a doctor is about treating patients as best as you can, and drawing appropriate reward (personal satisfaction is a form of reward) from doing so.
There are many previous generations of doctors who chose to let (or failed to stop) work taking over their lives. 50 years ago it was normal to eat, breathe and sleep medicine all day every day while you were a RMO or Registrar. Even as a GP in a solo practice it was normal. And your patients appreciated it. Doctoring was not a job, it was a lifestyle.
These days, nobody (in any profession) wants to make any personal sacrifices for the sake of work. We all want to clock off at the end of our shift, turn off our pagers and forget about work. And by that I don't mean just doctors, but everyone in the wider community. No longer is the community expectation "8 hours work, 8 hours rest, 8 hours sleep" (care of the trade union movement) but so is the 2 week overseas holiday, investment property, beach-house, private school education, 4WD, and token sustainable garden. Are we becoming a society of spoilt brats?
I increasingly see it in the surgical trainees (and I must confess that I am and was no exception). They don't want to move out of town for rural rotations, let alone interstate or overseas, for fear of disrupting their personal or family arrangements (neither did I, at that stage). They want to claim every single dollar of their award entitlements (as do I), though obviously this eats into the budget for treating patients. There is a cost and a benefit to each of these decisions - though self-interest increasingly outweighs that of community-interest.
But back to the point - if you want to give up your social life you will make significant professional and educational advances. If you want to prioritise your social life you will suffer some impediment to your career or study (in comparison to those geeks who don't sleep and talk med all day long). You may well live longer as well. BUT IT IS YOUR CHOICE.
Some people like to blame "the system" for making medicine stressful and demanding. Blame it all you like. "The System" is the way it is, and if you want to go into medical politics and change it for everyone else, it will have community-wide ramifications (not necessarily all for the better). A plethora of large and small organisations from the AMA to the DRS push their views on how to improve the health system and also working conditions for doctors.
Sometimes I don't know whether reform of the medical profession or medical employment is for the better or worse. I find it a rather ego-centric view that we have to demarcate roles, engage professional industrial representatives, or wage public campaigns in order to maintain wages and conditions for doctors.
It feels like we are stooping to a lower level, and that it demeans us as a profession that we have to engage in underhand tactics, or play hardball in order to maintain conditions. Every "victory" over some measly little payment or benefit seems to degrade my professional self-respect even more. Perhaps it says more about our government, our industrial landscape, or our lawyers. Most of all, it sickens me that the time spent on this detracts from what I want to do - treat my patients well.
I'd like to see someone stand up and say "Good Job, Doctors. Here's a pat on the back, a few days off, and a pay rise because you deserve it." But I know I'm just dreaming.
Now don't get me wrong, I am not against doctors having a social life and being able to wind down away from work. Heaven forbid, my family would be very unhappy if I completely ignored them to work all day and all night.
But this concept that doctors (and medical students) are entitled to a fun and enjoyable experience during their work or study irks me. Medical school is meant to get you trained up as a decent doctor... but it just so happens that all the students want it to be fun and enjoyable. Being a doctor is about treating patients as best as you can, and drawing appropriate reward (personal satisfaction is a form of reward) from doing so.
There are many previous generations of doctors who chose to let (or failed to stop) work taking over their lives. 50 years ago it was normal to eat, breathe and sleep medicine all day every day while you were a RMO or Registrar. Even as a GP in a solo practice it was normal. And your patients appreciated it. Doctoring was not a job, it was a lifestyle.
These days, nobody (in any profession) wants to make any personal sacrifices for the sake of work. We all want to clock off at the end of our shift, turn off our pagers and forget about work. And by that I don't mean just doctors, but everyone in the wider community. No longer is the community expectation "8 hours work, 8 hours rest, 8 hours sleep" (care of the trade union movement) but so is the 2 week overseas holiday, investment property, beach-house, private school education, 4WD, and token sustainable garden. Are we becoming a society of spoilt brats?
I increasingly see it in the surgical trainees (and I must confess that I am and was no exception). They don't want to move out of town for rural rotations, let alone interstate or overseas, for fear of disrupting their personal or family arrangements (neither did I, at that stage). They want to claim every single dollar of their award entitlements (as do I), though obviously this eats into the budget for treating patients. There is a cost and a benefit to each of these decisions - though self-interest increasingly outweighs that of community-interest.
But back to the point - if you want to give up your social life you will make significant professional and educational advances. If you want to prioritise your social life you will suffer some impediment to your career or study (in comparison to those geeks who don't sleep and talk med all day long). You may well live longer as well. BUT IT IS YOUR CHOICE.
Some people like to blame "the system" for making medicine stressful and demanding. Blame it all you like. "The System" is the way it is, and if you want to go into medical politics and change it for everyone else, it will have community-wide ramifications (not necessarily all for the better). A plethora of large and small organisations from the AMA to the DRS push their views on how to improve the health system and also working conditions for doctors.
Sometimes I don't know whether reform of the medical profession or medical employment is for the better or worse. I find it a rather ego-centric view that we have to demarcate roles, engage professional industrial representatives, or wage public campaigns in order to maintain wages and conditions for doctors.
It feels like we are stooping to a lower level, and that it demeans us as a profession that we have to engage in underhand tactics, or play hardball in order to maintain conditions. Every "victory" over some measly little payment or benefit seems to degrade my professional self-respect even more. Perhaps it says more about our government, our industrial landscape, or our lawyers. Most of all, it sickens me that the time spent on this detracts from what I want to do - treat my patients well.
I'd like to see someone stand up and say "Good Job, Doctors. Here's a pat on the back, a few days off, and a pay rise because you deserve it." But I know I'm just dreaming.
Thursday, January 10, 2008
First Day Tips for Surgical Interns
Every registrar or consultant has a talk that they give to new interns joining their team. It is about establishing heirarchy, rules, standard operating procedure, and team-building.
My talk generally incorporates a few important principles:
Apart from laying down the ground rules, I expect interns to learn along the way. There are many things that you have to work out for yourself, or are merely applications of common sense. Here are some tips:
A great deal of being an intern is learning to work within a team, being responsible for and to your patients, and getting yourself organised. These are skills that take time to develop - but they will come.
My talk generally incorporates a few important principles:
- Your job is to make my job easier. Just don't do anything illegal, unethical, or dangerous in order to do so.
- The consultants may mark your assessment form, but I tell them which boxes to tick.
- If I ask you a question about a patient, don't lie. If you don't know the answer, tell me that you don't know the answer.
- If I ask you to do something, I expect it done by the end of the day. If it isn't done, tell me why and when it will be done.
- Don't leave messages for me. If I am busy doing something, come and talk to me. If that means getting changed and coming into theatre, then do so.
- Decisions may be made on the ward round, but reasoning is discussed in the operating theatre. If you want to know why, come to theatre and listen.
- I expect an update at least once during the day and once at the end of the day. Don't go home without letting me know.
- Never be afraid to call me at any time - work, home or mobile. I would much rather know about an ill patient than a dead one.
Apart from laying down the ground rules, I expect interns to learn along the way. There are many things that you have to work out for yourself, or are merely applications of common sense. Here are some tips:
- Know What You Need To Know. Keep on hand a list of common phone numbers, pager numbers, and hospital stationery. Memorise the important ones. Know who your patients are and where they are at all times.
- Don't Shit Where You Eat. Nurses, Ward Clerks and Registrars that you need to make referrals to can make your life hell. Other interns will sometimes cover for you if you are busy. Keep them on your side. Sleeping with hospital staff (or patients) is a potential disaster area. Don't try it unless you are willing to cop the ensuing flak.
- Prioritise, Prioritise, Prioritise. Every ward round generates work. Usually a lot of it at once. Decide what is important, do what must be done immediately, and plan out your day so that the other tasks get done in a timely manner.
- Work Smarter, Not Harder. There are lots of time-saving ways to made your work efficient. Do things in batches. Keep pads of pre-filled pathology slips. Check results on all your patients together, not just one now and one later. Fill out Discharge Summaries ahead of time.
- Predict and Pre-empt. All units work on a timetable. Know the timetable, and what tasks need to be done before important events like unit meetings, ward rounds, and operating sessions. Repetition abounds. Start to recognise patterns in your registrar and consultant's behaviour in regards to certain patients, conditions, presentations etc. Predict what will need to be done and make preparations beforehand.
A great deal of being an intern is learning to work within a team, being responsible for and to your patients, and getting yourself organised. These are skills that take time to develop - but they will come.
Subscribe to:
Posts (Atom)




