"Nearly 50 per cent of the Australian surgical workforce is over 55 and is set to retire within the next 15 years, just as we start to experience the biggest ever demand for surgical services."
Really? I would imagine that most 55 year-olds would plan to retire within 15 years, and given that only practising fellows were surveyed the mean age of 55.5 years is probably not unexpected. Neither is the fact that 16 per cent of fellows are under 40. Nevertheless, I can't knock The Russter's activist attitude in righting the public misconceptions of surgical training in Australia. My favourite was this line from the press release:
"It takes 10 years to train a surgeon. You do the maths - we are running out of time."
What math? Sorry, you lost me there, Russ.
Understandably, most media outlets followed this up with fairly predictable reports:
- Doctors Warn of Surgeon Shortage, ABC 22/3/06
- Dad's army: half of all surgeons want to retire within 15 years, Sydney Morning Herald 22/3/06
- Where have all the surgeons gone?, NineMSN / Nine News 21/3/06
- Ageing crisis in surgery, Herald Sun 22/3/06
- Surgeon shortage crisis on horizon, The Advertiser 22/3/06
Not to stop there, 2 days later she decided to follow up with an article on Our Mate Vin but instead has muddied the waters further.
What concerns me (as I have said previously) is that I do not know whether reporters like Carol are merely ignorant of the issues truly facing specialist training (and is therefore being manipulated by political interest groups) or whether she is deliberately misrepresenting the situation for the purpose of newspaper sales.
Firstly, the university consortium is interested in expanding into all specialties, so why is the article a focus on "Battle over surgical monopoly"? Because surgeons make more interesting news than, say ... neuropsychiatrists. ("Who are neuropsychiatrists?", you may well ask. They are those doctors who, for example, would be interested in whether depressed people who think about ducks have more sensitive serotonin receptors in their amygdala - now try writing a front page news article about that!)
The other reason is that the ACCC has taken the trouble to investigate the RACS' role in surgical training - which makes you wonder why the ACCC targeted surgeons in the first place. At this point it becomes a revolving argument.
 Secondly, it is correct that Vin Massaro was CEO of the RACS from 1999 to 2003. I am not privy to his reasons for leaving the college or being hired by this university consortium, but it is just plain wrong to refer to him as "Uni push surgeon a college veteran". Our Mate Prof Vin is not a surgeon, or a medical doctor, but an academic with an interest in higher education policy. He worked very hard to represent the college of surgeons' interests when working with them, and now presumably works very hard to represent this consortium's interest (even if to the detriment of the college).
Secondly, it is correct that Vin Massaro was CEO of the RACS from 1999 to 2003. I am not privy to his reasons for leaving the college or being hired by this university consortium, but it is just plain wrong to refer to him as "Uni push surgeon a college veteran". Our Mate Prof Vin is not a surgeon, or a medical doctor, but an academic with an interest in higher education policy. He worked very hard to represent the college of surgeons' interests when working with them, and now presumably works very hard to represent this consortium's interest (even if to the detriment of the college).Thirdly, Our Mate Vin's submission to the ACCC as reported by Carol suggests that:
"The Commission should reconsider the involvement of medical schools in the training of specialists, through a parallel stream of training, so that new training pathways can be tested. These could include enabling students to begin their specialisation studies while undertaking their initial qualification thus reducing the length of the specialist training programs. Reducing the length of the training program would not directly affect the standard of clinical services or the quality of the graduates. Australia has a longer training program than the US and Canada (and now the UK), yet the standard of health care in those countries cannot be regarded as inferior to Australia's."
Perhaps Our Mate Vin should consider the fact that training systems in the UK are no shorter than in Australia, and that the latest revolution in US surgical traning is to implement schemes remarkably similar to (and almost as long as) those that exist here. And do you seriously believe that shorter and less training will not affect the quality of clinical services among graduates? I guess we can cut the medical course back from six years to four then... oh we have already done that. My bad.
At best I can only assume that the Vinster is not talking about shortening surgical training, but skipping internship and junior HMO jobs, where we learn the essentials of being a real-world doctor. Where we learn to respect the methods of our colleagues in other specialties, so that we can see the bigger picture when treating our patients. Where we can see and then decide which specialty we would actually consider working in. Where we act as the backbone of the public hospital system by doing all the day-to-day work like putting in IVs, writing drug charts, ordering and checking pathology and radiology tests, talking to patients and staying up all night to deal with those 3am acute febrile / hypertensive / nausea / insomnia / psychotic episodes. Yes, let's get rid of those doctors so that we can yo-yo the number of trainees in the pipeline temporarily.
But it does not take a rocket scientist to see that if I have to do 100 supervised rhubarbectomies to qualify as a rhubarb surgeon, and I only see 20 cases a year, then it will take... oh let's see, 5 years. So if we introduce an "alternative pathway" then my mate and I have to share the rhubarbs, and get 10 each a year... hang on, now I have to train for 10 years! How does that generate surgeons any faster? Oh, I see, we will just go to lectures on rhubarb theory and practise on rubber rhubarbs instead.
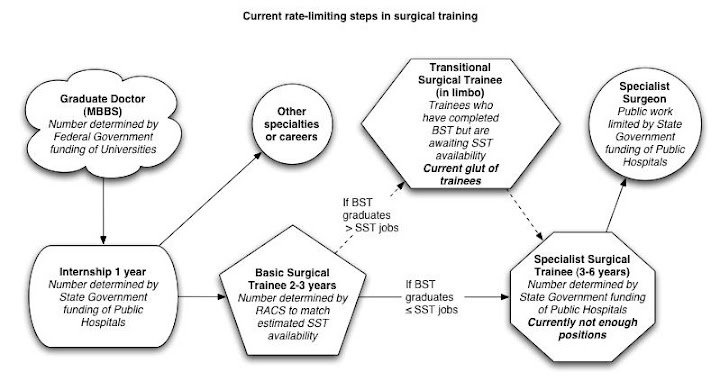
Fourthly, Old Vinnie Boy knows full well that the current rate-limiting step in the production of qualified, competent specialist surgeons is the provision of accredited training posts by the State and Federal Governments. He has said so himself. The State Governments have an interest in preventing basic surgical trainees from entering specialty training - that way they generate a glut of hospital medical officers, driving down salaries and conditions so that these doctors can have the privilege of being overworked and underpaid to give their all caring for patients. The Federal Government has an interest in limiting specialist numbers because this prevents patients having more access to surgery, procedures and drugs, all of which they would have to fund.
In a letter to federal Health Minister Tony Abbott this month, the universities said they hoped to start providing post-graduate specialist training as early as 2007. They will seek approval from the Australian Medical Council, which provides accreditation for training. They have also asked governments to fund training places in hospitals.
...
College of Surgeons president Russell Stitz said the college would be "quite happy" to work in partnership with universities, but said it would be unrealistic for them to become alternative providers at the moment. "They haven't got the capacity, they don't have surgeons that they can draw on, and how are they going to do it? Are they going to pay the surgeons? Because I can tell you the surgeons are not going to work for the universities for nothing."
Perhaps Our Mate Vin knows more than he is letting on... is setting up an "alternative pathway" code for "time to pay up, Governments"? The universities can only fund training if they start paying the trainers, something that the RACS has enough loyalty among fellows to avoid currently. All of that goodwill may evaporate soon if the current push to commodify surgical training continues. And given that accredited training jobs will not increase unless funding increases, any agreement by the Governments to fund university teaching will probably lead to a widespread funding increase to all parties (RACS, Hospitals and Universities). Somehow I think that ain't gonna happen.
Sadly, it is public perception (and that of the ACCC) that surgeons have a vested interest in limiting their own numbers. If that were so, we would not be giving up our time and energy pro bono (according to Russ-boy, $240 million worth a year) to train our colleagues, we would not be asking Government to fund more training positions, and we would be looking forward to our workload increasing, year by year, until we all died of exhaustion.
Perhaps it is against the tidal wave of public opinion, but I believe that surgeons, like all other doctors, have the primary goal of giving our patients the best possible care that we can provide.